
Orange County Facelift
Facelifts require a combination of a master plastic surgeon, a sculptor’s touch and an artist’s eye.
We encourage you to consider Dr. Arian Mowlavi for your Orange County Facelift. Accept only the best for your facial surgery.
An Orange County Facelift
demands a master plastic surgeon.
Orange County Facelift complements your facial features with a masterful facelift. e.

Get the facelift you want and deserve.
You have found the right Orange County Facelift Plastic Surgeon for the best possible results. A free consultation is the best place to start your journey.
Orange county facelift is dedicated to educating patients as the conclusive site for facelift surgery. Today surgeons offer a gamut of facial rejuvenation surgical options making choosing the best facelift even a more challenging endeavor. Today, facelift options include the skin only facelift, traditional facelift, extended SMAS facelift, short-scar facelift, or mini-lift. Moreover, we have to remember that the most effective facelifts should require lifting of the neck as well. This is because the face and neck are continuous with any skin redundancy extending through both areas. With the aging baby boomers, facelift surgeries are on the rise. In fact, over the last decade, there has been a 20 % increase in facelifts with approximately 100,000 facelifts performed annually. Even though non-invasive facial rejuvenation procedures have also risen in popularity, they have not matched the efficacy of the surgical facelift. As such the surgical facelift remains the Gold Standard amongst facial rejuvenation options. In order to discuss the nuances of facelift surgery, we must first discuss the facial anatomy.
Facial anatomy
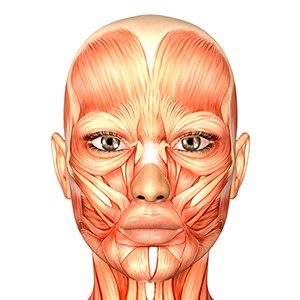
The facial soft tissues must be discussed in a three dimensional manner. Specifically, the face soft tissues must be described from superficial to deep and these tissues include the skin, superficial fat, the muscle fascia or lining, facial muscles, and the facial bones. The skin is the farthest away from the rigid facial bones and is most vulnerable to sagging. The superficial fat lies under the skin and is next layer to sag. The superficial fat is divided into compartments that are divided by specialized retaining ligaments. These retaining ligaments stretch between the skin and the underlying muscle fascia or lining and help structurally adhere the skin to the underlying muscles. These ligaments have been well described and include the zygomatic, the masseteric, and the mandibular ligaments. The zygomatic ligaments are located at the mid upper cheek and infra-orbital rim junction. The masseteric ligaments are located at the central mid cheek at the anterior border of the masseter muscles. The mandibular ligaments are located at the lower mid cheek at the border of the jawline. The next layer is the muscle lining, called the superficial myoaponeurosis system, i.e. the SMAS, which also droops with aging. Finally, the muscles of the face include the frontalis, the zygomatic, the masseter, the platysma, orbicularis oculi, orbicularis oris, and the lip depressor muscles. The muscles are least likely to sag because they are intimately attached to the rigid facial bones.
| Facial Muscles | Function | Innervation |
| Frontalis | Elevates the eyebrow | Frontal nerve |
| Orbicularis Oculi | Closes the eye | Frontal nerve |
| Zygomaticus Muscles | Lifts the corner of the mouth | Zygomatic Nerve |
| Orbicularis Oris | Closes the mouth | Buccal Nerve |
| Platysma | Lifts the neck | Cervical Nerve |
| Depressor oris | Pulls the corner of the lip down | Marginal mandibular Nerve |
These above facial muscles and the major facial muscles and innervated by the five facial motor nerves. The facial nerves travel mostly on the undersurface of the facial muscles but on occasion may rise superficial to the muscles and lie underneath the SMAS. This anatomic nuance of the facial nerve is what makes facelift surgery technically challenging. In fact, the SMAS, the muscle fascial layer or lining, remains the most critical component to superior facelifts offered by facelift specialists. Specifically, expert facelift surgeons are able to undermine and lift this layer in addition to the skin and superficial layer to improve the leverage of pull on the skin and soft tissues but meanwhile taking extraordinary care to avoid injury to the facial motor nerves.
Before we discuss the available options in facelift surgery, we must describe the anatomic changes that occur with facial aging. Aging changes involve continued growth of skin and soft tissues and development of subsequent redundancy in facial and neck skin. When we combine skin redundancy with the continued effects of gravity, we start seeing the undesirable aesthetics of sagging skin and soft tissues. This means sagging of the skin, superficial fat, and SMAS. If we observe the aging face and neck changes we will appreciate specific concern areas. The first aging sign includes skin redundancy and soft tissue fullness of the neck especially over central neck under the chin. Additionally, the platysma muscle that spans across the neck can split causing vertical platysma bands that are visible when smiling. Next, along the jawline, skin and soft tissue can fall down and centrally and bunch up against the mandibular ligament and are called jowling. Additionally, the corner of the lips will often become downturned. The medial cheek skin will fall down and bunch up centrally against the massater ligament at the nasolabial fold. Finally, the lateral cheek and lower lateral eyelid skin may also fall down and bunch up centrally against the zygomatic ligament. Now that we have reviewed the aging changes as they relate to the facial anatomy, we can discuss the various maneuvers that have been proposed to correct them.
Skin only facelift
The skin only facelift utilizes traditional incisions that start at the temple, follow the front of the ear, then on the back of the ear and on to the hairline. The facial skin is dissected up to the anterior masseter in order to free up the nasolabial fold and across the neck to free up the redundant neck skin. The redundant skin and superficial fat is then undermined, lifted up, trimmed, and incision line repaired. The main advantage of the skin only lift is that it can be done while you are awake. However, the skin only lift is considered a suboptimal lift in that it can appear operated and unnatural in appearance. This is because all of the tension of the lift is placed on the skin layer. In addition, since all of the tension is placed on the skin, incision lines are prone to hypertrophic scarring and the ear can become pulled forward creating a paisted on earlobe appearance, coined the Pixie ear deformity.
Mini facelift
The mini facelift is a limited skin only facelift that minimizes the length of the incision line to the front of the ear only. As such, it can only tighten the facial skin in the mid and lower face. It will not achieve any rejuventation of the upper cheek nor any improvement of the neck. It has been promoted as the lunch time facelift and advocated to patients that are only interested in minimizing their surgical and recovery commitment. Unfortunately, this facelift is considered the least effective of all of the facial rejuvenation surgeries.
Traditional facelift
The traditional facelift utilizes full length incisions as described in the skin only facelift that allows the surgeon to complete full undermining of the face and neck skin as described above. Additionally, the SMAS muscle lining is tightened with a stitch, called plication, or following conservative elevation prior to stitching of the SMAS, called imbrication. The reason for conservative elevation of the SMAS is the concern over inadvertent injury to a facial motor nerve discussed above. The traditional facelift does require more aggressive anesthesia using intravenous or general anesthesia since the dissection plane under the SMAS can be uncomfortable. However, the traditional facelift is considered the mainstay of facelifts and neck lifts for most plastic surgeons.
Short-Scar Facelift
The short-scar facelift utilizes traditional facelift techniques but with an incision line limited to the front of the ear only. As such, it can only effectively treat facial skin redundancy and is unable to effectively treat the neck. It should be reserved for patients in their late 30s or early 40s who have minimal skin redundancy and no neck skin redundancy.
The Extended SMAS Facelift
The extended SMAS facelift is considered the GOLD STANDARD in facelift techniques. It utilizes a full length incision technique that allows for correction of the upper, middle, and lower cheeks, the jawline, as well as the neck regardless of the severity of skin redundancy and degree of sagging. It’s unique in that it requires an extended dissection of the SMAS to the zygomatic retaining ligaments such that the entire upper, middle, and lower skin can be fully mobilized. More aggressive dissection of the SMAS does require expertise in facial anatomy and surgical skill such that facial motor nerve injury is avoided. As such this facelift is only offered by 10 % of surgeons and it does require general anesthesia. In contrast to other techniques, the extended SMAS facelift provides definitive, long term, correction of facial aging changes, in a natural and smooth manner.
An Orange County Facelift Should Include a Neck Lift
Patients with severe neck skin laxity will require either traditional or the extended SMAS facelift technique to maximize neck skin mobilization and tucking. When fat excess is present, then liposuction must be supplemented to the pull of the skin. If the neck muscle, called the platysma, is torn in the central neck region, then vertical platysma bands may be noticed when the patient flexes his orher neck muscles. Up to 25 % of patients may demonstrate partial or complete platysma tears. When a platysima tear is detected, then a generous incision placed under the neck can be used to access the bands and repair the plastysma muscle in the midline.
The importance of the SMAS and why it defines the Orange County Facelift
The SMAS layer is integral to superior facelifts since it provides pull of the overlying facial skin without leveraging the tension on the skin itself. This important consequence is why patients that are treated with the dual plane SMAS and skin layer facelifts do not look operated looking as described by coined descriptions of the joker mouth, the windblown eyes, and the Pixie ear deformity. The joker mouth describes an overly tightened corner of the lips. The windblown eyes describe an overly tightened corner of the eyelids. Finally, the pixie ear deformity describes the paisted on earlobe appearance. In addition, by taking the tension off of the skin layer, your incisions will heal without prominent scars. Finally, by virtue of tightening the soft tissues with the SMAS layer, you will provide a smooth base to lay down the skin on thus avoiding unnecessary lumps and bumps. One of the secrets to achieving these benefits of the SMAS lift is to limit undermining of the skin to the anterior border of the massater to avoid complete release of the skin from the SMAS in the mid cheek so that the SMAS can remain attached to and pull up the cheek skin. This ensures leveraging and partial suspension of the skin lift to minimize tension on the skin layer. Whereas zygomatic ligaments may be divided the masseteric ligaments are kept intact. Traditional facelifts elevate the SMAS up to zygomaticus ligaments and stay lateral to anterior parotid gland in comparison to the extended SMAS facelift which elevates the SMAS just past the zygomaticus origin and beyond anterior border of parotid gland until zygomatic ligaments are divided and even the masseteric ligaments mobilized. A survey of facelift surgeons has found that SMAS plication is performed by 37 % of surgeons, conservative SMAS undermining and tightening by 17% of surgeons, and extended SMAS undermining by only 10% of surgeons.
Avoiding facelift complications
Avoiding complications during facelift surgery is critical to ensuring successful facelift outcomes. The most common danger of facelift surgery is development of a blood pocket in the dissected tissue planes, called a hematoma. A hematoma is caused by oozing of microvessels that have been irritated by tissue dissections and is dangerous because if it is not treated immediately it can cause pressure on the skin flaps and cause skin compromise. Hematomas can be eliminated with both appropriate preoperative planning as well as strict compliance in the postoperative period. In the preoperative period it is critical to avoid all blood thinners for at least a month that include Aspirin like products, supplements such as Omega-3 fatty acids, fish oils, Ginko Boloba, and foods such as fish, almonds, and turmeric. In the postoperative period, you must control your blood pressure by staying on your medications if you have hypertension, and avoid bending down to tie your shoes, losing your temper, or holding your breath. Another complication can occur if facial motor nerves are compromised intraoperatively. Intimate knowledge of facial nerve anatomy can help your surgeon avoid nerve injuries. The most common injured nerve is the greater auricular nerve that provides sensation to the lower part of the ear. This nerve exits the neck muscles approximately 6 cm below the ear and travels up to the ear getting more superficial as it nears the ear. Injury to this nerve can be avoided by making the skin flaps thinner when close to the ear. In addition, when tightening the SMAS under the ear, a SMAS flag shaped flap is created to span over this nerve and thus avoid stitching in this region. The next nerve that is prone to injury is the frontal branch that helps you raise your eyebrow and close your eyes. This nerve can be injured when dissecting the upper aspect of the SMAS over your cheek bone. As a result, the dissection of the SMAS is limited superiorly to avoid injuring this nerve.
Facelift Recovery
Facelift recovery is fairly seamless as long as you are compliant with your surgeon’s instructions. When you awake from surgery, you will find your head and neck wrapped in a surgical bra. This bra has several roles and these include ensuring that your dissected neck and face skin heals back down. In addition, the compression of the bra helps prevent hematomas described above. Remember to avoid blood thinning medications, herbs, and food groups. As well, make sure you avoid raising our blood pressure and make sure to take your hypertension medications if you are ne them. You will also find small drains that are secured temporarily and act as a safety net. As we have discussed above, if you should happen to get a hematoma, the drains will help remove the blood so that you don’t develop unnecessary compression and skin compromise. These drains are usually removed by one week following surgery. In addition, the sutures in front of the ear are removed at one week and your neck sutures are out by day 10 to 12. This means that you can expect to go out to dinner with family and friends as early as 12 days following surgery. You should refrain from physical activities for one month. If you are going to do any public speaking or attend an important event, plan to have your surgery at least a month prior to your event.
Facelift Summary
In general, undergoing a facelift is a very successful facial rejuvenation surgery and a tolerable journey. The gold standard extended SMAS dual plane facelift is performed in approximately 2.5 hours. When you awake you will be comfortable and have a surgical bra in place. You may need a few pain pills but only for the first few days. Patients are asked to sleep with their heads elevated for the first week. Finally, all facelift patients are asked to have a responsible adult present over the first two days to keep an eye out for them. Remember that facelift patients will feel functional throughout their recovery and be expected to walk around and tend to their daily needs. If patients have any facelift surgery concerns, they are encourage to contact our office so that we can provide them more information.